This is Dr Robert Malone, who invented the mRNA vaccine. He has some advice for parents and grandparents who are being asked to have their children ‘jabbed’ against Covid.
Virus
Covid Conundrums
Have you ever wondered why some people do not want to be ‘jabbed’? Or do you need to explain to others why you do not want to be ‘jabbed’? We live in strange times when people who have chosen to be ‘protected’ from Covid19, by having two ‘jabs’, are worried about meeting people who have not been ‘vaccinated’. If the vaccines work, what do they have to fear? If the ‘so-called’ vaccines do not work, why should anybody have them? We seem to have reached the extraordinary situation where the ineffectiveness of these vaccines is blamed upon the people who have not had them. I do not claim to cover all the angles but in this post I list many of the points which I believe should be open for discussion. The mainstream media, however, never allows any of these topics to be raised.
[All the references in this post can be found on the Covid-References page]
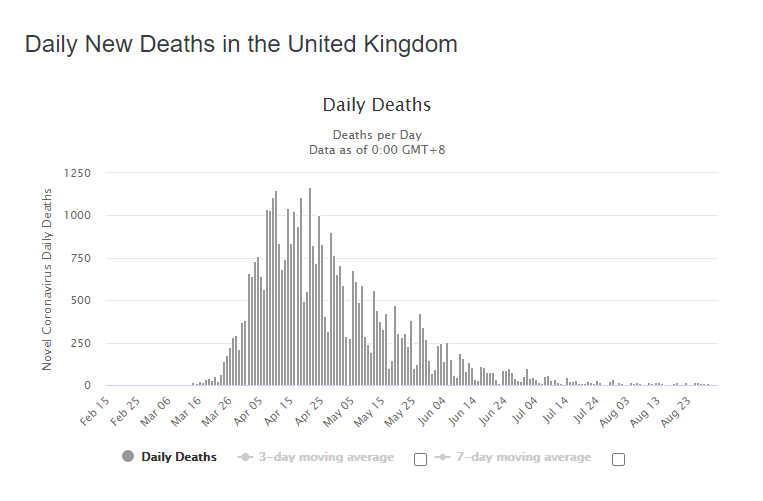
1.Falsification of numbers. The daily reporting of deaths was used to scare everybody into believing SARS-Cov-2 was an extremely deadly virus. But the totals were for people who had died ‘within 28 days of a positive Covid test’. This has never been done previously for any other disease. It includes all the people who died of cancer, heart disease, road accidents and suicide as long as they had a recent positive test. Nobody knows how many have died specifically of Covid because this is a deliberate falsification.
2. The Government listened to the advice of Prof Ferguson, who predicted a death toll of half a million people. A cursory glance at the history of Ferguson’s previous clairvoyance shows a constant, reliable record of enormous over-exaggeration. He has never come close to being correct. [Ref 1] The Government used a totally unreliable source to guess at the possible severity of the disease and caused panic by giving it credence.
3. The media fearmongering was enhanced by the daily reporting of ‘case’ numbers, which were determined by the PCR test. However, the PCR test was not designed as a diagnostic tool. The polymerase chain reaction is a method of replicating a segment of genetic material and when the process is repeated sufficiently often there is enough material for it to be detected. Detecting a fragment of viral DNA via this method cannot possibly tell you if it came from a living, active virus or the remnants of a dead virus, which has been destroyed by the individual’s immune system. To suggest that all PCR positive results are from infectious people is false. [Ref 2]
4. During the first wave, the median age of death was 82, which is slightly older than the national, UK, median age of death at 81 years of age. [Ref 3] Figures issued by the ONS (Office for National Statistics) showed that 95% of the people who died with Covid had pre-existing disease. [Ref 4] It was clear from the beginning that this virus was only dangerous to the elderly and those with compromised immune systems. Not one person in the Government or Sage has recommended steps to improve metabolic health and our immune systems. They have totally ignored all the evidence that deficiencies in vitamin D, zinc and selenium are closely linked to a weakened immune system. [Ref 5] The correct diet, or appropriate supplementation, cannot carry a downside and, for most people, will help. This has never been mentioned by the people employed to advise on our health.
5. Lockdown. The quarantine of infected, ill people has been shown to reduce the spread of infectious diseases. The quarantine (lockdown) of millions of healthy people has never been used before and has no medical history to recommend it. The Government enforced this experiment on the nation without any attempt to perform a risk-to-benefit analysis. If Boris Johnson worked for a private corporation and had introduced such draconian, expensive and experimental measures without any attempt to calculate the unforeseen consequences, he would have been sacked for dereliction of his duty. The idea that lockdowns worked and should have been implemented earlier has gained widespread acceptance, without any evidence for their benefit. Data from each of the States in America shows no significant difference between the states which locked down and those that did not. [Ref 6]
6. A considerable surge in early deaths occurred in care homes. This was caused by the incompetent, and Government led, removal of large numbers of hospitalised, unwell people back to care homes which were not equipped to deal with them. Many of these unfortunate people had Do Not Resuscitate notices applied to them without their consent. [Ref 7] There is some evidence that many of these were ‘finished off’ with the excessive use of Midazolam injections, stocks of which were ordered by Matt Hancock. [Ref 8]
7. The Strategic Advisory Group for Emergencies (Sage) is a committee whose members change depending upon the nature of the current emergency. The Chief Medical Officer, Chris Whitty, and The Chief Scientific Adviser, Patrick Vallance, chose the people they believed are best suited to help the Government to make appropriate decisions. The group they assembled contained no expert immunologists but it did contain several mathematical modellers and behavioural scientists. As a consequence, the country has been subjected to a grotesque series of psychological stresses and fears. [Ref 9] Professor Sheldon Cohen of the Carnegie Mellon University is an expert in the effect of stress on immunity. He has shown that prolonged isolation and fear are hugely detrimental to our ability to resist respiratory viruses. [Ref 10] It is as if lockdowns were designed to make us all less able to fight off viruses with our natural immunity. If Sage did not know this, they are negligent and if they did know but still proceeded with lockdown, they are corrupt.
8. The Sage group also contains an extraordinary number of conflicts of interest tied to the Pharmaceutical Industry and especially to vaccine manufacturers. They have constantly promoted vaccines and ignored all other possibilities. It is well known that natural immunity after infection provides better and longer lasting protection from reinfection than that provided by vaccines. But Sage and the Government have continually insisted that everyone must be vaccinated regardless of whether they have naturally produced antibodies or not. This makes no medical sense but makes huge financial profits for vaccine producers. [Ref 11]
9. For several months in the spring of 2020 Sage told us there was no reliable evidence to support the wearing of masks to reduce transmission. However, masks were made mandatory in July 2020 precisely when the prevalence of this seasonal virus had reached its lowest level of the year. Boris Johnson tells us he is following the science but clearly nobody is. The logical reason for implementing a mask mandate in summer is to maintain the fear already created by lockdowns. [Ref 12]
10. I referred to ‘so-called’ vaccines earlier because these ’jabs’ are not strictly vaccines. They are a type of medical device, which creates a protein in the body and this protein elicits an immune response. A typical vaccine consists of a dead or harmless virus which directly produces an immune response to the entire virus. A typical vaccine is also expected to prevent an individual from contracting the disease and from transmitting it. The Covid jabs allow you to catch Covid and transmit it. Their only claim to benefit consists of a promise that a Covid infection will be less severe than if you had not had the jab. How can they quantify that? How do they know how one individual would have reacted to Covid with or without the jab? This is not a deadly disease; the chance of survival is exceptionally good. [Ref 13]
11 These ‘vaccines’ are pushed hard on to absolutely everybody but they have not finished their trials yet, and do not do so until 2023. They have received ‘Emergency Authorisation’ which is not full approval. To obtain Emergency Authorisation, a medicine must be the only viable option during a clear and obvious emergency. The only health emergency in the UK is metabolic syndrome, which consists of obesity, heart disease, diabetes and high blood pressure. [Ref 14] Sixty-four per cent of the population are overweight and we know, from 4 above, that metabolic disorders greatly increase an individual’s risk of serious Covid complications. Metabolic diseases are the reason the NHS is constantly under pressure. Throughout their tenure, neither Whitty nor Vallance have done a single thing to improve the nation’s metabolic health.
Emergency Authorisation cannot be granted if there is an alternative therapy. Sage, the Government, and the media have ignored all other treatments and disparaged any that have been mentioned. Ivermectin is a safe and cheap drug which has been taken by millions of people for years. There is considerable evidence from around the world that it is effective against Covid19. [Ref 15]
12. We have already seen that Covid poses no danger to healthy young people, but the age group at which people are ‘invited’ to have a ‘jab’ continues to fall. When it reached schoolchildren, the JCVI (Joint Committee on Vaccination and Immunisation) decided to recommend against ‘jabbing’ such young people because the benefit did not outweigh the risk. Chris Whitty and the other home nation CMOs decided to ignore expert advice and proceed. (We have already seen that Whitty has serious conflicts of interest when it comes to the promotion of vaccines.) Before having any medical procedure, an individual is supposed to give informed consent. It is also contrary to the Nuremburg Code to use coercion to persuade someone to have a medical procedure. The Government’s entire campaign of persuasion towards young people has involved coercion, with constant reference to ‘getting your freedoms back’ and without any mention of the undeniable risks involved with this ‘vaccine’. The Government’s actions are unethical and immoral.
13. Covid jabs have a terrible safety record. [Ref 16] All previous vaccines have been withdrawn when they displayed harm to recipients of lesser degree than these do. The latest VAERS report shows extraordinary levels of damage, but it receives no publicity in the mainstream media. These results would normally cause a vaccine to be banned from use. Why don’t they? Government data on ‘variants of concern’ from August 2021 shows that you are more likely to die from Covid if are double vaccinated than unvaccinated. See [Ref 17]
14. Since the emergence of Sars-1 and MERS many years ago, the pharmaceutical industry has been trying to produce an effective coronavirus vaccine. All attempts have failed during the animal trials because of a reaction known as ADE (Antibody-dependent enhancement). [Ref 18] The vaccines initially created antibodies but when the animals were challenged by a wild virus, the disease was made worse by the over-reaction of the immune system. (This may be what is happening with Ref 17.) What many sceptical people find truly sinister is the desire to ‘jab’ every single person in the world with a ‘vaccine’ that has not been through any animal trials and was rushed into use via Emergency Authorisation. The unvaccinated are, in fact, performing the vital role of a control group, which is something the authorities do not want. Why would that be?
15. The ‘vaccine passport’. Scotland has already introduced a mandatory vaccine passport, creating a medical apartheid that most of us thought could never happen in the UK. England will no doubt follow soon. This will bar all unvaccinated people from their inalienable rights and all normal gatherings for theatre, sport and social events. If Covid19 was a deadly disease and the vaccine prevented infection and transmission, it might make sense. But it is clear that Covid is not particularly dangerous for the vast majority of healthy people and the vaccine neither protects from infection nor transmission. So vaccinated people can gather and possibly infect each other but unvaccinated people will not be allowed to gather even if they have recently tested negative. Does this sound like they are following the science? Or does it sound like Covid is being used as an excuse to introduce a system of digital control over our lives, where we all have to ‘show our papers’?
Do you think any of the points I have raised are, at least, worthy of a civilise debate on television? If so, why do you think that debate never happens?
Gross negligence by Sage

According to the latest Ispos MORI poll, confidence in the ability of the NHS to deal with people suffering from Covid-19 has declined. Their latest press release stated, “A clear majority of Britons are confident in the ability of the NHS to deal with those who are ill as a result of the virus, but this has fallen 12 points from November and now stands at the lowest level since the pandemic began. Meanwhile 35% are not confident the NHS can cope, up 11 points from November. Confidence is split along party lines, those favourable to the Conservatives are significantly more likely to be confident in the ability of the NHS to deal with the Coronavirus (72%) than those favourable to the Labour Party (56%).”
It seems inevitable that people will worry about the NHS becoming overwhelmed when we are told, every day, that this is happening. The only surprising thing about this poll is the degree to which people’s confidence in the health service is so partisan. People seem to believe their favourite political party can make the NHS work well, even though 99 per cent of MPs have no scientific background.
I believe there are more important questions to ask than the one used in this poll. For instance, ‘have the Government and Sage done everything they can to alleviate the danger of Covid infections?’, and ‘have the Government and Sage done a thorough analysis of the benefits compared to the harms of prolonged lockdowns?’ The answer to both these questions is a resounding no.
Covid-19 is a nasty, and sometimes, fatal disease for those who become infected. I believe it is sufficiently virulent that a nationwide effort to tackle it is entirely appropriate. However, to say I am disappointed by the response would be a huge understatement. In my opinion, what the Government and Sage have done, and more importantly have failed to do, amounts to gross negligence. These are some of their failings:
The UK suffers from very high rates of obesity, type 2 diabetes and other components of metabolic syndrome. These diseases are caused by chronic, elevated blood sugar, which leads to insulin resistance. This enormous problem has been putting the NHS under pressure for decades. Doctors working independently, and contrary to official guidelines, have been able to reverse these conditions, without medication, by the adoption of a low carbohydrate diet. The authorities have made no attempt to change dietary guidelines despite relevant evidence from all over the world. This failure is vitally important because 95% of people who have died with Covid-19 had pre-existing conditions, which were mainly metabolic disorders. This hugely significant fact has been ignored.
Published research has shown that raised blood sugar increases your risk of dying with Covid. Here is a quote from the study, “The cumulative probability of mortality was significantly higher in patients with hyperglycaemia compared to patients with normoglycaemia, independently of pre-existing diabetes.”
Other work has shown that high levels of fructose, which is part of the table sugar molecule, inhibits the ability of immune cells to recognise viral and bacterial pathogens. If our defences cannot see a virus, they cannot fight it.
The effect of metabolic disorders on Covid mortality is also demonstrated by variations in the gut biome. Prevalence of certain bacteria predicted which patients would die from Covid with 96% accuracy. Those bacteria in question proliferate in people with poor diets and poor health.
If the health authorities had used the viral epidemic to advise everyone to avoid ultra-processed food, sugar and refined carbohydrates they could have avoided thousands of Covid deaths and simultaneously reduced the burden of metabolic diseases, from which millions of people suffer.
There is no good evidence that lockdowns work in the long run. However, there is clear evidence that prolonged lockdowns make the entire population more susceptible to severe symptoms when they catch a respiratory virus. Professor Sheldon Cohen has worked for decades on the relationship between prolonged stress and more severe viral infections. He regards chronic social isolation and fear as the most potent stressors for damaging the immune system. Inevitably, lockdowns increase social isolation and fear. Perhaps the new coronavirus variants are not more transmissible; they just seem to be so because now we are all more susceptible.
No harm-to-benefit analysis has been performed for lockdowns, which demonstrates staggering ineptitude and negligence. Other researchers, however, have done this work and state any benefit does not warrant the harm and lockdowns should be eased. People have died in their homes for fear of going to hospital; some have died of cancer because their treatment was curtailed; some have committed suicide because their businesses and lives have been ruined. Psychologists are extremely concerned about the life-altering mental damage caused to millions of young people.
The vast majority of people infected with Sars-CoV-2 do not need hospital treatment, and do not die, because their immune system defeats the virus. The robustness of our immunity is weakened by metabolic syndrome and stress, as mentioned above. However, simple steps can be used to enhance the function of our immune system.
Many people have Vitamin D deficiency in the winter. This study, among many others, shows that those with the lowest level were far more likely to die of Covid19 than those with optimum levels. Supplementation is cheap and readily available. There is no downside to having optimum levels of vital nutrients. People have died of Covid because of Vitamin D deficiency. During the summer we were allowed to exercise outdoors but not allowed to sit in the sunshine, even when alone. This prevented the accumulation of vitamin D stores. Other factors which boost immune systems and general health include a diet of real food, exercise, and good sleep. None of these have been mentioned.
Oxford University have announced they are starting a trial to test the efficacy of the drug Ivermectin. We do not need a trial because we already have robust evidence that Ivermectin is of considerable benefit to seriously ill Covid patients if administered early. Why are they delaying the use of this important, cheap drug?
I would like to see MORI conduct a new poll asking, ‘How confident are you that Sage are doing everything they can to reduce the impact of the virus?’ I wonder what the results would be if they only ask the people who have read the references quoted here.
Vitamin D and disease
Chris Whitty and Patrick Valence have consistently failed to mention the potential benefits of adequate Vitamin D levels in Covid19 patients. The following links are a sample of references relating to Vitamin D and infectious diseases, which those two senior medical advisers should be aware of. Sensible supplementation with Vitamin D carries no risk but can be of great benefit. There is no excuse for not making this information available.
https://pubmed.ncbi.nlm.nih.gov/27714929/
https://pubmed.ncbi.nlm.nih.gov/20067648/
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2770157
https://www.medrxiv.org/content/10.1101/2020.09.04.20188268v1.full.pdf
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7455115/
https://www.mdpi.com/2072-6643/12/9/2757
http://www.societaitalianadiendocrinologia.it/public/pdf/hypovitaminosis_d_covid19.pdf
Covid Testing and Cases

The media is still full of horror stories about Covid19. The Government is still imposing local lockdowns and international quarantines in and from a constantly changing array of locations. The fear of this viral disease is rampant and constantly maintained by the mandatory wearing of face masks so that wherever we go we are reminded that our fellow humans may be dangerous. The graph below of Daily Deaths shows that for the last two months there have been almost no deaths related to the Coronavirus. So why do we suffer all this loss of liberty?
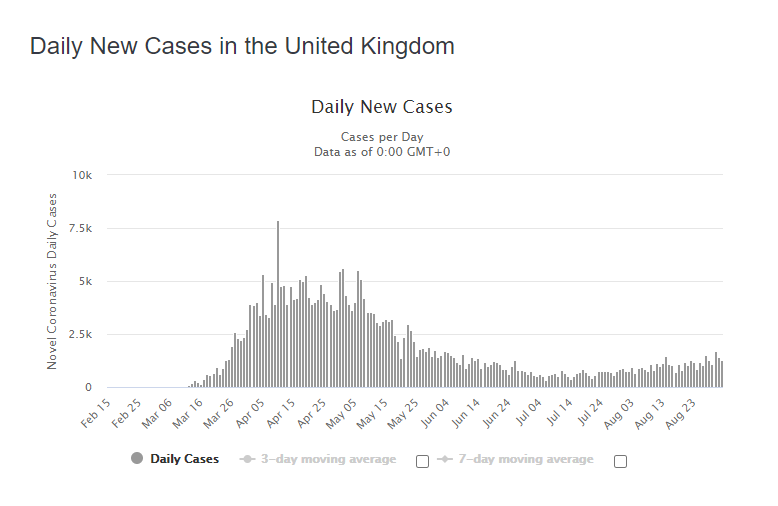
The story has changed. We used to hear about the number of people dying but now we only hear about the number of new cases. We are told that new cases mean the virus is spreading and, even if we have no symptoms, we could be giving it to someone who will die. As we can see in the Cases graph below numbers diminished steadily from April to mid June but have since risen slowly. The media want us to believe that the “second wave” is coming and we will have to lockdown all over again. However, there is another explanation.
During March and April, when the virus was peaking, people who were clearly ill and hospitalised were the only ones tested. When they all started getting better, the ‘Test and Trace’ idea became prevalent. This involves testing as many people as possible, especially those who may have had contact with someone else who has tested positive. When more people are tested more positive test results will be found. Does this mean the virus is spreading? The answer is not necessarily because of what the test is actually looking for. The PCR test involves taking a swab of the back of the throat and nostrils. The swab is then tested for genetic material from the virus. Remnants of viral RNA can remain in the body for weeks, or even months, and can be detected by this very sensitive test. Therefore, if you had the virus 5 weeks ago you can still test positive but you are neither infected nor infectious.
Most of these new cases are in people who are asymptomatic, but if you have no symptoms you have no illness. The definition of ‘illness’ is to be in poor health or sickness. All these cases are irrelevant if the people are not ill.
Michael Mina is an Epidemiologist, Immunologist & Physician at Harvard School of Public Health & Harvard Medical School. On August 21, 2020 he wrote this to explain the sensitivity of PCR tests for Covid19 and how they are able to give a positive result for people who are no longer infected nor infectious.
1/The molecular tools we use like PCR for #COVID19 tests detect the virus genome. Like detecting DNA in a piece of hair, detecting virus RNA tells little about whether the virus is still active…
2/When the virus is growing and someone is transmitting virus, it grows to billions of viruses. So it’s easy to detect when virus load is high using antigen tests (look for the virus proteins themselves) or PCR (look for the RNA) …
3/But after the virus is cleared by the immune system, all of those viruses leave little trails of RNA behind. The RNA gets stuck in vesicles on the cells and it can sit there, in the nose or mouth, for weeks or months at very low levels…
4/So what does this have to do with a super sensitive PCR test being too sensitive that it can potentially cause more harm than good…?
5/The PCR test can continue picking up that leftover RNA the whole time it is there – for weeks or months AFTER the viral infection has been essentially cleared. So ultimately, the majority of time spent in the PCR positive state is after infection, not transmissible
6/So this can be harmful if testing is very infrequent like it is in the US (most people get tested only once, if ever – but even if testing every few weeks)The idea of the super sensitive PCR test is to detect people when at low viral load at the beginning of infection
7/But if screening tests are only every few weeks, the chances you detect someone in the very short window of time between turning PCR positive and having 10x higher viral loads (the virus grows fast and exponentially inside the body) is very slim. This window is hours.
8/On the other hand, with a very sensitive test, people might stay positive for many weeks or even months because it continues to detect the leftover RNA from the past infection. But this can be bad – it leads to unnecessary quarantines of people already past their infection
9/ If doing low frequency screening of asymptomatic people with PCR, the majority of people found to be positive will be detected only after their infection. So in the US we are unnecessarily quarantining millions of people, assuming they are infected when they’re already recovered
10/And we are contact tracing all of these people and quarantining and testing their contacts looking only at the two days prior to their swab for the test – meanwhile they were likely infectious 1-5 weeks earlier! So wasting resources tracing the wrong people.
11/To sum, we are using extremely sensitive PCR tests for screening. They are expensive and limited so we do them very infrequently. What we gain is ability to find someone a few hours earlier – only IF by chance the swab is taken in the few hours where it makes a difference
12/What we lose is ability to more frequent tests and thus do not catch people when it matters. Further, we mistakenly end up quarantining millions of people for 10 days because we erroneously assume any PCR + test was collected at the beginning of an infection. When most are after.
13/So maybe the most sensitive PCR test is not only costly for screening, but maybe even more damaging than a cheaper more frequent lower sensitivity test. The apparent missed cases maybe aren’t false negatives. Maybe the (+) on the PCR are False (+) for actionable results
14/I think it’s time we take a hard look at the types of tests we are using, what they do and do not tell us about infection, and figure out how to use them accordingly, instead of just assuming that more sensitive is better. Maybe less sensitive is better for some things.
15/ To finish, high sensitivity PCR is great if you are a doctor and need to know what is wrong with your patient. Like a detective, you want all shreds of (RNA) evidence. But it’s not always better & sometimes a lower sensitivity test is more accurate at detecting active infection. We published on some of these issues as well as how the viral load data from the PCR could be better used clinically earlier this year: “To Interpret the SARS-CoV-2 year, consider the Cycle Threshold Value”
Thousands of people have lost their jobs; businesses have closed; depression, suicides and paranoia are on the rise; cancer patients go untreated; children are frightened, unschooled and masked; we are not allowed to have parties or go to watch sport; we are suspicious of our fellow humans; we have sacrificed so many freedoms for the sake of ….. what? We are doing this for a rise in test results that show that people who are not ill had a virus at some time. This is not okay. This is not science. This is an agenda and it is not for our benefit. We need to complain and fight back.
Coronavirus and diet
I wrote a tweet recently comparing the extraordinary global response to Covid-19 and the total lack of response to the millions of people who die each year because of metabolic syndrome. Several people replied that you cannot compare the two because one is infectious and the other is not. They suggested that we cannot do anything about the virus but we can all chose to improve our metabolic health. I wasn’t comparing the diseases; I was comparing the response to them. Metabolic disease will kill more people this and every year than Coronavirus but the authorities make no bold efforts to examine the reasons for those deaths.
There are a few important things to add to this debate.
- The majority of people who die from this virus are elderly and already have metabolic diseases. One of the most common of these is type 2 diabetes, which is avoidable with the correct diet. Metabolic disruption makes people more vulnerable to the virus.
- The best way for any of us to avoid succumbing to the virus, or fight it off without needing hospitalisation, is to have a first-class immune system. Several factors affect our immunity and the most important is diet.
- The virus causes death by attacking the lungs and causing respiratory failure.
Vitamin D: This study finds evidence that higher levels of vitamin D help to reduce respiratory tract infections. – Vitamin D for prevention of respiratory tract infections
Vitamin A: This study shows the importance of adequate levels of vitamin A for correct lung function. Vitamin A Deficiency and the Lung
Both of these vitamins are fat soluble and likely to be low in people on a low-fat diet. They can also be low in people on a vegetarian or vegan diet because the best sources are in animal-based foods:
Vitamin A
Beef and lamb’s liver, salmon, tuna, mackerel, butter, cheese, eggs
Vitamin D
Salmon, tuna, herring, sardines, eggs, lard and bacon fat.
Of course, the best source of vitamin D is from sunlight on our skin (without sunscreen). However, during a British winter, it is not possible to get enough sunshine to create adequate amounts of this essential substance and we have to get it from our diet. It is worth remembering that it is a cholesterol molecule that is converted to vitamin D in the skin. Eating a lot of plant sterols (or taking statins) will reduce levels of cholesterol and potentially lower our immunity.
Diabetes I mentioned earlier that many of the fatalities are among people with diabetes. This study shows why that may not be a coincidence. Glycolytic control: A mechanism to regulate influenza viral infection
This is a quote from the Abstract of the study: “As new influenza virus strains emerge, finding new mechanisms to control infection is imperative. In this study, we found that we could control influenza infection of mammalian cells by altering the level of glucose given to cells. Higher glucose concentrations induced a dose-specific increase in influenza infection.”
A low-carbohydrate diet, as recommended on this site, has many more benefits than just weight loss and reversal of type 2 diabetes.
Minerals Some trace minerals have a profound effect on the integrity of our immune systems. Three of the most important ones are thought to be Zinc, Iodine and Selenium. They only occur in decent amounts in whole, unprocessed foods. Processing greatly reduces the mineral content.
Zinc is quite well-known for fighting the common cold. It is found in meat, shellfish, lentils and beans, nuts, dairy and eggs.
Iodine is essential for thyroid function and the thyroid is important for immunity. There are few good sources of iodine but the best include cod, tuna, shrimp, eggs, dairy, iodised salt and seaweed!
Selenium is an antioxidant that we require in trace amounts. Too little causes problems but so does too much. It is better to eat healthy foods than take supplements that may provide too much. The best sources of selenium are brazil nuts, pork, beef, chicken, cottage cheese, eggs, mushrooms and spinach.
Good metabolic health, weight, blood sugar and an excellent immune system all come from eating the diet we evolved to eat: a low-carbohydrate diet of mainly animal-sourced protein and fat. What we eat can definitely improve our chances of fighting off the worst effects of Coronavirus. Why is the Chief Medical Officer not telling us this?